Perhaps the biggest misunderstanding about how skeletal muscles function to produce the body’s movements concerns their particular role. Most people think that a muscle performs ONE particular and very defined role and that they always perform this role. This is not how it works. Muscles must work together to produce different bodily movements and a particular muscle’s role may change depending on the movement.
Synergy and Synergist Muscles
The most important aspect to understand about how muscles function to produce a joint movement is synergy. Synergy means that two or more things work together to produce a result that is greater than any of those things could do alone so that the whole result is greater than the sum of the individual effects of the agents involved.
Even the simplest joint movement requires muscles working together in this synergistic or cooperative fashion. When a group of muscles work together to optimally perform a given motor task this is known as a muscle synergy. These synergies are of utmost importance in biomechanical research and physiotherapy. 1Knudson, Duane V. “Chp. 3: Anatomical Descriptions and Its Limitations.” Fundamentals of Biomechanics. New York: Springer, 2007. 57-58. Print.,2Whiting, William Charles., and Stuart Rugg. “Muscular Control of Movement and Movement Assessment.” Dynatomy: Dynamic Human Anatomy. Champaign, IL: Human Kinetics, 2006. 121. Print.

Agonist and Synergist Muscles
Usually, the muscles that are directly involved in producing a certain joint movement are called agonists and muscles that are indirectly involved, by some other role, are called synergists. However, even if a muscle adds directly to a joint’s movement by adding its own torque, it can still correctly be called a “synergist”. Other muscles, such as stabilizers, neutralizers, and fixators, that help the movement by opposing unwanted movement or by helping to stabilize the joint are also synergists.
Synergists
So, the word “synergist” is not a very useful word, in itself, when describing muscular roles since it is much too inclusive, and the way it is used is contradictory to its definition as it excludes muscles that could rightly be called synergists by their “synergistic” role in a joint movement. This happens when all the muscles involved in a movement besides the prime movers are termed synergists as if the prime movers themselves are not synergists. These muscles that contribute to a movement indirectly could more clearly be called supporters.
Students of strength training are always having great difficulty in distinguishing the difference between agonists, synergists, stabilizers, fixators, etc. Muscle synergy, as above, is an important concept, but the word synergist, used to describe a muscle’s role, is a silly word that is used in different ways by different texts. We’d do well to abandon it.

Although the word is not useful, it is largely used so we cannot simply ignore it even though we could easily side-step it by simply describing the different roles a muscle may take in helping to produce a movement. But, this would simply cause more confusion, not less, and it is not my place, here as StrengthMinded, to decide whether the term should be abandoned. It is used in two slightly different ways, depending on the precise definition of the word
- A synergist is an agonist that is not directly responsible for the movement of a joint but assists in some other fashion
- A synergist is another muscle, besides the agonist, that assists the movement of a joint indirectly
Do not be too surprised by this. As you study human movement you will find contradictions to be the rule. It is not always completely decided how terms should be used and, to be frank, many of the most popular usages are incorrect ones.

The first definition we can easily render incorrect, as will be seen since it incorrectly uses the word agonist to include muscles that cannot be considered agonists. The second definition is better as it uses the word agonist correctly but it still uses the confusing word synergist, which we have to deal with. So, we will deal with it by accepting it but insisting upon using it properly. Therefore, we will say that a muscle that indirectly assists in producing a joint movement is the agonist’s synergist. So from here on out, the term synergist will become agonist’s synergist. Don’t worry about the unwieldiness of this since, for the most part, we can simply avoid the word altogether as it adds little to any discussion of muscle actions.
While some muscles work together, in a concentric fashion, to produce a movement, others work in other ways to help cancel out other movements, such as the unwanted movement of another bone that the muscle attaches to, or by opposing the movement that could occur in an undesired plane of motion. The movement produced is the net result of all the different forces produced by the muscles.
Agonist Muscle (Prime Mover)
As stated above, agonist muscles are muscles that are responsible for causing a certain joint motion. However, the term is often defined incorrectly to mean ALL the muscles that have a role in producing a movement. By this definition stabilizers, neutralizers, and fixators are also agonists. This is incorrect.
An agonist is a muscle that is capable of increasing torque in the direction of a limb’s movement and thus produce a concentric action. In other words, the muscle can produce a force that accelerates a limb around its joint, in a certain direction. This does NOT mean that this direction is the only one the muscle can produce force in but only that it is capable of this and thus is directly involved in producing a certain movement, making it a prime mover.
To keep it simple, then, an agonist is a muscle that causes rotational movement at a joint by producing torque. A movement can always have more than one agonist although a certain agonist may be capable of producing more torque than its partner. They are also sometimes called protagonists.

Agonist vs. Prime Mover
Many people refer to muscles having a redundant role in producing torque about a joint as being synergistic agonists but with one of these muscles being the prime mover. This is a silly and arbitrary distinction since there are many instances where a muscle with a redundant role can take over for a paralyzed one, making that muscle the “prime mover”. Agonist and “prime mover” simply speaking, means the same thing and the terms are interchangeable.
However, sometimes it is useful to refer to one muscle, usually a larger one that articulates at more than one joint, as the prime mover. In this way, the prime mover can be spoken of in relation to its fixators or supporters. This type of instance is very common in that certain terms only become useful in a specific context. The biceps brachii, which will be used as an example from here on, is often considered the prime mover in elbow flexion, although it is only one of several flexors of the elbow joint.
The brachialis, for instance, is another elbow flexor, located inferior to the biceps on the upper arm. Unlike the biceps, which inserts onto the radius, which is able to rotate, the brachialis inserts onto the ulna which cannot rotate. This, it can be said that the brachialis is the only pure flexor of the elbow joint whereas the larger biceps can also supinate the forearm.
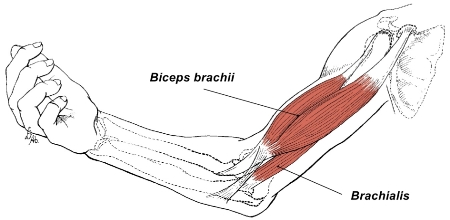
think of the more superficial biceps brachii.
But the brachialis is the only pure elbow flexor.
A muscle can only be referred to as an agonist in relation to a movement or another muscle. It is never proper to call any one muscle an agonist unless we are describing its role in a movement or we are referring to it in terms of a muscle on another side of the joint, known as an antagonist. To say “the biceps is an agonist” is incorrect or at least incomplete (which comes down to the same thing). 3McGinnis, Peter Merton. “The Muscular System.” Biomechanics of Sport and Exercise. Champaign, IL: Human Kinetics, 2005. 259. Print.
The biceps brachii is an agonist for elbow flexion. It is assisted by the brachialis and the brachioradialis. These are the agonists of elbow flexion, all of which are capable of flexing the elbow joint to some extent.
Agonist’s Synergists Roles: Stabilizer, Fixator and Neutralizer
Some muscles involved in a joint action do not directly contribute a torque force to the movement but assist the movement in indirect ways. These are roles that are commonly referred to as synergist muscles, as explained above, but that we are calling the agonist’s synergists. These roles are many but some of the basic terms used to describe these muscles are stabilizer, neutralizer and fixator. However, the term stabilizer, for our purposes, means the same thing as fixator. The term stabilizer needs further clarification before we move on to the fixator.

Stabilizers and Stabilization
There is more than one way to categorize the functional role of muscles. It depends on perspective. We may look at the muscles in terms of their function in specific movements or we may look at them in terms of the entire body as a system, complete with many subsystems. The latter view is not what we are concerned with in this explanation but the when viewed this way muscles are classified according to their function rather than their role in a particular movement. The word stabilizer or stabilization, therefore, has a much broader and complex definition.
This view sees the body as a system of motor (or mobilizer) and stabilizer muscles. This concept was first proposed by Rood and furthered by the work of Janda and Sahrmann as well as by Comerford and Mottram who proposed the concept of local and global stabilizers and global mobilizers. 4Middleditch, Alison, and Jean Oliver. “Muscles of the Vertebral Column.” Functional Anatomy of the Spine. Edinburgh: Elsevier Butterworth-Heinemann, 2005. 96-97. Print.
Although, the concept of a stabilizing muscle can still be viewed in terms of a single movement in this system, certain muscles are considered to have the primary function of stabilizers in the body, being, by virtue of their position, shape, angle or structure, more suited to work as a stabilizer than as a mobilizer.
Although its complexities go way beyond the scope of this explanation (and the expertise of its author), this way of looking at the body is a valid and important one for the strength trainee. For instance, this view teaches us that the abdominal group of muscles, once primarily thought of as a muscle we perform situps with, is much more important as a major stabilizer of the spine. This lesson may lead us to train those muscles in a way that supports their function, thus making us stronger and more injury free. This, in fact, is one of the hallmarks of “functional” training, although the term has been much abused and overused.

The type of stabilizer we will discuss here, however, are fixators, which are active during one movement and at one joint. There are certain muscles that act primarily as stabilizes because of their angle of pull. An example of such muscles is a group of muscles known as the rotator cuff muscles of the shoulder girdle. This group comprises the supraspinatus, infraspinatus, teres minor and subscapularis. These muscles are mainly known as muscles of rotation for their contribution to external and internal rotation of the shoulder but they are actually much better suited for the primary role of stabilization and they are very important in stabilizing the humeral head in the glenoid fossa.
What is Angle of Pull? A muscles angle of pull is the angle between the muscle insertion and the bone on which it pulls. This is the angle at which the muscle force acts relative to an axis or lever. Given the equation for torque: τ = rF sin θ, and the angle of pull of the muscle being the angle θ, the larger the angle of pull, the larger the resultant torque produced by the muscle. For more detailed explanation see Applied Biomechanics: Concepts and Connections by John McLester and Peter St. Pierre.
Fixator Muscle
A fixator is a stabilizer that acts to eliminate the unwanted movement of an agonist’s, or prime mover’s, origin.
Many muscles are attached to more than one bone. When this happens the muscles are said to be multiarticulate or multi-joint muscles. When these muscles contract they tend to move both bones to which they are attached. This would, of course, make everyday movements quite impossible.
For instance, consider elbow flexion by the biceps brachii. When you do a curl, the biceps acts to flex the elbow. However, the biceps is attached at two places, proximally and distally. Its distal attachment, the insertion, is to the radius. It’s the radius bone we want to move when we curl a dumbbell. One of its proximal attachments, though, the origin, is to the scapula. The scapula is one heck of a mobile bone. In fact, it has no real bony attachments of its own.
When the biceps contracts it will tend to draw the radius and the scapula together. The movement of the scapula must be prevented. This is accomplished by fixators. Specifically, the trapezius and rhomboids work isometrically to keep the scapula from moving on the torso. 5Pitt-Brooke, Judith, and Heather Reid. “Musculoskeletal Requirements for Normal Movements.” Rehabilitation of Movement: Theoretical Basis of Clinical Practice. Edinburgh [etc.: W. B. Saunders, 2004. 97-99. Print.
Neutralizer Muscle
Neutralizers, like fixators, act to prevent unwanted movement. But instead of acting to prevent the unwanted movement of a body part they act to pull against and cancel out an unwanted line of pull from the agonist or prime mover. Many muscles can produce a pulling force in more than one direction so that an undesired joint action may occur simultaneously with the desired one. Neutralizers prevent this.
For example, the biceps brachii can do more than flex the elbow. It can also supinate the forearm (twist the forearm so that the palm faces up). In order for biceps action to flex the elbow without the forearm also being supinated another muscle must cancel out the supination torque that the biceps also produces. The pronator teres, being the principal forearm pronator, is responsible for this.
Test the action of the pronator teres for yourself. You can easily palpate the pronator teres by flexing your elbow and making a fist as if you are holding a hammer (this is a “neutral” forearm position). The pronator teres will start to contract. You can feel it with your opposite fingers inside the middle of your forearm. Now, relax your forearm and bring your hand up toward the ceiling. You will feel the pronator teres relax and lengthen. At first, it was contracting to provide a pronating force against the biceps supinating force while the elbow is flexed. When you supinated your forearm, it relaxed to allow this action to take place.
On the other hand, if forearm supination were desired without elbow flexion, the triceps would act isometrically to resist the flexion, making it a neutralizer.
Antagonist Muscle
An antagonist is a muscle that is capable of opposing the movement of a joint by producing torque that is opposite to a certain joint action. This is usually a muscle that is located on the opposite side of the joint from the agonist. The triceps, an extensor of the elbow joint, is the antagonist for elbow flexion, and it would also be correct to say that the tricep is an antagonist to the biceps, and vice versa.
In order for an agonist to shorten as it contracts the antagonist must relax and passively lengthen. This occurs through reciprocal inhibition, which is necessary for the designated joint movement to occur unimpeded.
Reciprocal inhibition is a neural inhibition of the motor units of the antagonist muscle. When the agonist muscle contracts, this causes the antagonist muscle to stretch. Normally, this stretching would be followed by a stretch reflex which would make the muscle being stretched contract against the change in length. If this were allowed to happen unchecked then it would result in very jerky or oscillatory movement since the stretch reflex in the antagonists would elicit a new stretch reflex in the agonist, so on and so forth.
These types of oscillatory movements are sometimes able to occur after damage to ascending motor pathways, causing repetitive alternate contraction of agonists and antagonists. This is called clonus and is probably due to spinal inhibitory interneurons not functioning properly. The inhibition of the alpha-motoneurons in the antagonist are brought about by Ia-inhibitory interneurons of the spinal cord, which are excited by IA afferents in the agonist muscle. 6Brodal, Per. “Chp. 21: Peripheral Motor Neurons and Reflexes.” The Central Nervous System Structure and Function. New York: Oxford UP, 2010. 292-93. Print.
However, antagonists are not always inactive or passive during agonist movements. Antagonists also produce eccentric actions in order to stabilize a limp or decelerate a movement at the end of a motion. For instance, during running the hip extensors are antagonists to the hip flexors, which act to bring the femur forward during the running stride.
So, the hip extensor muscles must relax to some degree to allow this forward motion of the thigh to take place. However, the extensors must also act to arrest this forward motion at the top of the stride. So the antagonists both relax to allow the motion to happen and then contract to put the brakes on it. This makes for a very fine balance of activity between agonist and antagonist pairings. 7McLester, John, and Pierre Peter. St. “Chp. 11: Biomechanics of Muscle Location, Origin and Insertion.” Applied Biomechanics: Concepts and Connections. Belmont, CA: Thompson Wadsworth, 2008. 327-29. Print.

Agonist Antagonist Coactivation or Co-contraction
When both the agonist and antagonist simultaneously contract this is called coactivation. It can be advantageous for coactivation to occur for several reasons. For instance, when movements require a sudden change in direction, when heavy loads are carried, and to make a joint stiffer and more difficult to destabilize.
The purported reason that co-contraction may occur during changes in direction is that modulating the level of activity in one set of muscles is more economical than alternately turning them on and off. For heavy loads, increased joint stiffness is desirably for lifting heavier loads and co-contraction of the core muscles of the torso routinely occurs during these activities. For fine motor activities of the fingers, as well, complex co-contraction activity is needed.
It should be noted that the word co-contraction is only used to describe the simultaneous activity of agonist/antagonist parings and should not be used to describe the simultaneous action of various agonist muscle groups. 8Whiting, William Charles., and Stuart Rugg. “Muscular Control of Movement and Movement Assessment.” Dynatomy: Dynamic Human Anatomy. Champaign, IL: Human Kinetics, 2006. 121. Print.,9Alter, Michael J. “Neuroscience of Flexibility.” Science of Flexibility. Champaign, IL: Human Kinetics, 2004. 82. Print.
Spurt and Shunt Muscles
Muscles can also be described as being spurt or shunt muscles. These roles are largely unknown in the strength training world but are described in the orthopedic and physical therapy fields. Again, we will consider the elbow joint.
When a muscle acts on a bone it actually produces a force that, if one were to do a vector analysis, could be resolved into two component forces. These components are an angular component and a transarticular component. The angular component is actually the perpendicular or vertical component of the muscle’s force. We normally call this the rotary component. If allowed to act alone this force would cause the bone to rotate around the joint. The rotary component is also known as a swing component.
The transarticular component is a parallel or horizontal component. It acts along the shaft of the bone and may produce a force that pulls the bone away from the joint or toward it, depending on the angle of the joint. This component, therefore, is also known as either a stabilizing component or a destabilizing component. When the component is stabilizing it is also known as a shunt component and shunt muscles are muscles that tend pull the bones of a joint together.
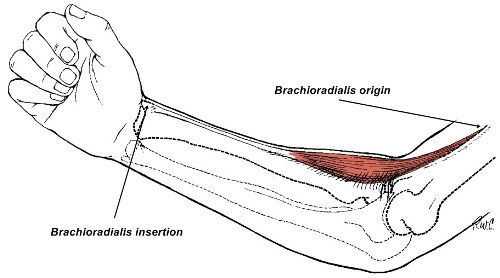
During elbow flexion, the angular component, the one that makes the radius move around the elbow joint, is the swing component. The brachioradialis is an example of a shunt muscle, which is able to provide a compressive force.
A certain muscle may exert a stronger spurt or shunt force. If the spurt force is stronger it is called a spurt muscle. If the shunt force is stronger it is called a shunt muscle. Which happens depends on the location of the muscle and whether the distal or proximal attachment is free to move.
Generally, the distance of the origin and insertion of a muscle to the joint axis of rotation determines whether a muscle acts as a spurt or shunt muscle. When the distance of the insertion is greater than the distance of the origin, the muscle is considered a shunt muscle. When the origin is farther from the joint axis than insertion, the muscle is a spurt muscle. This is important because a shunt muscle may protect a joint from powerful distracting or compressive forces during certain movements. 10Kulkarni, G. S. “Muscle: Structure and Function.” Textbook of Orthopedics and Trauma. New Delhi: Jaypee Brothers, 2008. 79-80. Print.,11Pitt-Brooke, Judith, and Heather Reid. “Musculoskeletal Requirements for Normal Movements.” Rehabilitation of Movement: Theoretical Basis of Clinical Practice. Edinburgh [etc.: W. B. Saunders, 2004. 97-99. Print.,12Rybski, Melinda. “Chp. 4: Factors Influencing Strength.” Kinesiology for Occupational Therapy. Thorofare, NJ: Slack, 2004. Print. A shunt muscle could be considered a stabilizer muscle as it help to stabilize a joint during movement.
You should be able to visualize, using the image of the brachioradialis above, how the insertion distance allows such a muscle to exert a shunt or stabilizing force on the bone and joint regardless of the joint angle. Imagine a dumbbell curl with the elbow flexed to greater than 90 degrees. The brachioradialis, like most of the elbow flexors, will pull the bone toward the elbow joint at this angle. However, imagine what would happen if the insertion were much closer to the elbow rather than all the way down at the end of the radius at the wrist.
As the angle of elbow flexion passes 90 degrees this same parallel pull is no longer pulling the bone toward the joint but is pulling the bone away from the joint, resulting in a translational or dislocating force. But since the insertion is so distant, at the wrist, the angle of elbow flexion does not affect the direction of the parallel component and it remains a shunt component, making the brachioradialis a shunt muscle, always able to exert a stabilizing force. See further explanations of this in the comments below this article.
If you need to learn more about muscle roles and other aspects of biomechanics and kinesiology, a very good text to start with is Biomechanics of Sport and Exercise by Peter McGinnis.


{kind=link}

Resources
| ↲1 | Knudson, Duane V. “Chp. 3: Anatomical Descriptions and Its Limitations.” Fundamentals of Biomechanics. New York: Springer, 2007. 57-58. Print. |
|---|---|
| ↲2, ↲8 | Whiting, William Charles., and Stuart Rugg. “Muscular Control of Movement and Movement Assessment.” Dynatomy: Dynamic Human Anatomy. Champaign, IL: Human Kinetics, 2006. 121. Print. |
| ↲3 | McGinnis, Peter Merton. “The Muscular System.” Biomechanics of Sport and Exercise. Champaign, IL: Human Kinetics, 2005. 259. Print. |
| ↲4 | Middleditch, Alison, and Jean Oliver. “Muscles of the Vertebral Column.” Functional Anatomy of the Spine. Edinburgh: Elsevier Butterworth-Heinemann, 2005. 96-97. Print. |
| ↲5, ↲11 | Pitt-Brooke, Judith, and Heather Reid. “Musculoskeletal Requirements for Normal Movements.” Rehabilitation of Movement: Theoretical Basis of Clinical Practice. Edinburgh [etc.: W. B. Saunders, 2004. 97-99. Print. |
| ↲6 | Brodal, Per. “Chp. 21: Peripheral Motor Neurons and Reflexes.” The Central Nervous System Structure and Function. New York: Oxford UP, 2010. 292-93. Print. |
| ↲7 | McLester, John, and Pierre Peter. St. “Chp. 11: Biomechanics of Muscle Location, Origin and Insertion.” Applied Biomechanics: Concepts and Connections. Belmont, CA: Thompson Wadsworth, 2008. 327-29. Print. |
| ↲9 | Alter, Michael J. “Neuroscience of Flexibility.” Science of Flexibility. Champaign, IL: Human Kinetics, 2004. 82. Print. |
| ↲10 | Kulkarni, G. S. “Muscle: Structure and Function.” Textbook of Orthopedics and Trauma. New Delhi: Jaypee Brothers, 2008. 79-80. Print. |
| ↲12 | Rybski, Melinda. “Chp. 4: Factors Influencing Strength.” Kinesiology for Occupational Therapy. Thorofare, NJ: Slack, 2004. Print. |